
De Quervain’s tenosynovitis
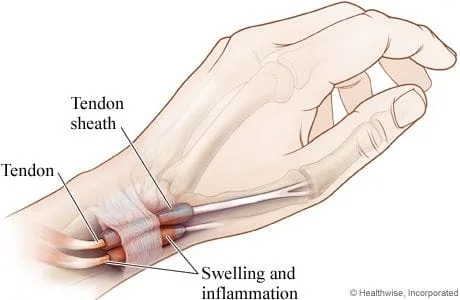
De Quervain’s tenosynovitis is an inflammation of the tendons and synovial sheaths of two muscles in the forearm: the abductor pollicis longus and extensor pollicis brevis. De Quervains tenosynovitis results from repetitive friction and microtrauma causing the tendons and sheath to swell, making normal motions painful.
Predisposing movements include lifting, grasping and pinching, particularly when combined with wrist radial or ulnar deviation. These activities force the tendons to rub. Activities like gardening, knitting, cooking, playing a musical instrument, carpentry, walking a pet on a leash, texting, video gaming and sports like golf, volleyball, fly fishing and racquet sports are known culprits (2,4-6).
The condition was once known as “Washer woman’s sprain”, since wringing out wet clothes is a known trigger. (7) Lifting infants & children by placing an outstretched finger and thumb beneath their armpit has led to the nicknames of “Mommy thumb” or “Baby wrist”. This problem affects a significant number of new mothers during the post-partum period wherein involvement is often bilateral. (8,11)
Symptoms of Dequervain’s:
Symptoms include pain on the lateral aspect of the wrist. The pain may begin abruptly but more commonly is of gradual onset, increasing over weeks or months. Pain may travel towards the elbow. The pain is provoked by movement of the thumb or hand, especially forceful pinching, grasping or twisting. Visible swelling over the tendon area is common. Presence of a fluid-filled cyst in this region is possible. Patients may complain of a slight “squeaking” sound or sensation associated with movement of the wrist. Catching or snapping is possible.
Do I need imaging?
Typically the answer is no. Ultrasound is useful for diagnosing tenosynovitis and identifying the presence of an intracompartmental septum. (24-26) MRI is an alternative. Imaging of tenosynovitis patients should be reserved for those with a history of trauma or other red flags and in those who fail an initial trial of conservative care.
Treatment options:
Initial anti-inflammatory measures may include ultrasound, cryotherapy, NSAIDs, and rest.
Patients should avoid activities that provoke pain.
Video game players and those who text should take frequent breaks and hold their wrists straighter.
Patients should limit pinching, gripping and twisting.
IASTM may be implemented judiciously to release adhesions in the associated tissues.
Soft tissue manipulation and myofascial release techniques may be needed for the affected muscles as well as the wrist extensors and brachioradialis.
Therapeutic taping may provide benefit.
Manipulation of wrist and/or cervical restrictions is appropriate. For patients who do not respond to a brief trial of conservative therapy, cortisone injection is effective in about 80% of cases (17,32)
Surgery is rarely necessary and should be reserved for patients who fail conservative treatment and cortisone injections.
At Creekside Chiropractic & Performance Center, we are highly trained to treat this condition. We are the only inter-disciplinary clinic in Sheboygan county that provides chiropractic, myofascial release, ART (Active Release Technique), massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiropractor in Sheboygan by the Sheboygan Press.
Evidence Based-Patient Centered-Outcome Focused
Sources:
1. Peters-Veluthamaninal C, Winters JC, Groenier KH, Mayboom-deJong B. Randomized controlled trial of local corticosteroid injections for de Quervain’s tenosynovitis in general practice. BMC Musculoskel Disorders. 2009;10:131
2. Retig AC. Athletic injuries of the wrist and hand. Part II: overuse injuries of the wrist and traumatic injuries to the hand. Am J Sports Med. 2004;32(1):262–273.
3. Dawson C, Mudgal CS. Staged description of the Finkelstein test. J Hand Surg. 2010;35A(9):1513–1515.
4. www. physio-pedia.com/De_Quervains_Tenosynovitis, August 2013
5. Ashurst J.V., Turco D.A., Lieb B.E. Tenosynovitis caused by texting: an emerging disease. J Am Osteopath Assoc. 2010 May;110(5):294–296.
6. Rossi C., Cellocco P., Margaritondo E., Bizzarri F., Costanzo G. De Quervain disease in volleyball players. Am J Sports Med. 2005 Mar;33(3):424–427.
7. Wolfe SW: Tenosynovitis. In Green DP, editor: Operative hand surgery, Vol. II, Philadelphia, 1999, Churchill Livingstone.
8. The Wall Street Journal, The Baby May Be Giving You Mommy Thumb Tuesday, December 7, 2010
10. Ann R Coll Surg Engl. 2007 April; 89(3): 326–327.
11. Vuillemin V, Guerini H, Stenosing Tenosynovitis, J Ultrasound. 2012 February; 15(1): 20–28
12. Lapidus PW, Fenton R: Stenosing tenovaginitis at the wrist and fingers: report of 423 cases in 369 patients with 354 operations. Arch Surg 64: 475, 1952.
13. Louis Patry, Michel Rossignol; Guide to the diagnosis of work- related musculoskeletal Disorders; Edition Multimonde, 1998
14. Wolf JM, Sturdivant RX, Owens BD. Incidence of de Quervain’s tenosynovitis in a young, active population. J Hand Surg Am. 2009;34:112–115.
15. Jackson WT, Viegas SF, Coon TM, Stimpson KD, Frogameni AD, Simpson JM. Anatomical variations in the first extensor compartment of the wrist: a clinical and anatomical study. J Bone Joint Surg Am. 1986;68:923–926.
16. Kulthanan T, Chareonwat B. Variations in abductor pollicis longus and extensor pollicis brevis tendons in the Quervain syndrome: a surgical and anatomical study. Scand J Plast Reconstr Surg Hand Surg. 2007;41:36–38.
17. Lee Marilyn Peterson, Nasser-Sharif, Zelouf David: Surgeon’s and Therapists Management of Tendonopathies in the Hand and Wrist, Hunter J, Mackin E, Callahan A, Rehabilitation of the Hand, 5th ed. Vol. l, pp. 931-933.
18. Fournier K, Bourbonnais D, Bravo G, Arsenault J, Harris P, Gravel D. Reliability and validity of pinch and thumb strength measurements in de Quervain’s disease. J Hand Ther. 2006;19(1):2–10.
19. Kirkpatrick William H, Lisser Steven: Soft tissue conditions:Trigger fingers and De Quervain’s syndrome: Hunter J, Mackin E, Callahan A, Rehab of the Hand 4th ed. Vol. II, pp 1012-1014.
20. Goubau JF, Goubau L, Van Tongel A, et al. The wrist hyperflexion and abduction of the thumb (WHAT) test: a more specific and sensitive test to diagnose de Quervain tenosynovitis than the Eichhoff’s Test J Hand Surg Eur Vol January 22, 2013
21. Dawson C, Mudgal CS. Staged description of the Finkelstein test. J Hand Surg. 2010;35A(9):1513–1515.
22. Malanga GA, Nadler S. Musculoskeletal physical examination: an evidence-based approach. Philadelphia, PA: Elsevier Mosby; 2006. pp. 171–173.
23. Alexander RD, Catalano LW, Barron OA, Glickel SZ. The extensor pollicis brevis entrapment test in the treatment of de Quervain’s disease. J Hand Surg Am. 2002;27(5):813–6.
24. Grassi W, Lamanna G, Farina A, Cervini C. Synovitis of small joints: sonographic-guided diagnostic and therapeutic approach. Ann Rheum Dis1999;58:595
25. Kwon BC, Choi SJ, Koh SH, Shin DJ, Beek GH. Sonographic identification of the intracompartmental septum in de Quervain’s disease. Clin Orthop Relat Res. 2010 Aug;468(8):2129–34.
26. Diop AN, Ba-Diop S, Sane JC, Tomolet Alfidja A, Sy MH, Boyer L, Badiane M. Role of US in the management of de Quervain’s tenosynovitis: review of 22 cases[French] J Radiol. 2008 Sep;89(9 Pt 1):1081–4.
27. Witt J, Pess G, Gelberman RH: Treatment of de Quervain tenosynovitis: a prospective study of the results of injection of steroids and immobilization in a splint, J Bone Joint Surg 73:219, 1991.
28. Weiss AP, Akelman E, Tabatabai M: Treatment of DeQuervain’s syndrome, J Hand Surg 19:595, 1994.
30. Nyska M, Floman Y, and Fast A: Osseous involvement in de Quervain’s syndrome, Clin Orthop 186:159,1984.
32. Richie CA, Briner WW., Jr Corticosteroid injection for treament of de Quervain’s tenosynovitis: a pooled quantitative literature evaluation. J Am Board Fam Pract. 2003;16(2):102–106.
33. Kulthanan T, Chareonwat B. Variations in abductor pollicis longus and extensor pollicis brevis tendons in the Quervain syndrome: a surgical and anatomical study. Scand J Plast Reconstr Surg Hand Surg. 2007;41:36–38.
34. D'Angelo K, Sutton D, Côté P, Dion S, Wong JJ, Yu H, Randhawa K, Southerst D, Varatharajan S, Cox Dresser J, Brown C, Menta R, Nordin M, Shearer HM, Ameis A, Stupar M, Carroll LJ, Taylor-Vaisey A. The Effectiveness Of Passive Physical Modalities For The Management Of Soft Tissue Injuries And Neuropathies Of The Wrist And Hand: A systematic Review By The Ontario Protocol For Traffic Injury Management (optima) Collaboration. J Manipulative Physiol Ther. 2015 Aug 21.