
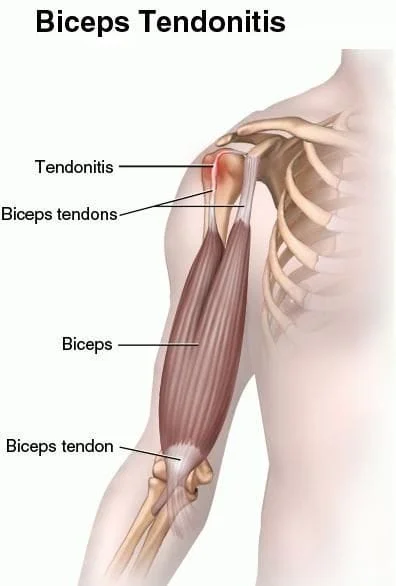
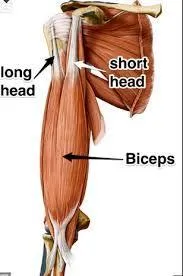
Biceps tendinopathy:
Biceps tendinopathy describes a painful inflammation or degeneration of the tendon of the long head of the biceps. (1,2) The term “tendinopathy” may suggest either an inflammatory or degenerative origin. (3) In the case of a recent insult, inflammation (tendinitis) may be a valid explanation. However, current evidence suggests that many cases of tendinopathy occur without inflammation and are the result of chronic overload, which leads to microscopic tearing, failed healing and degenerative changes within the tendon. (3) Injuries that have been present over three months consistently demonstrate fibrosis and degeneration with very little actual inflammation (3).
Who is most likely to have a biceps tendinopathy?
Biceps tendinopathy is most common in young adults between the ages of 18 and 35. (12) The condition often results from repetitive overhead activity, including throwing, swimming, gymnastics, martial arts, racquet sports, and contact sports (12-13). Subacromial impingement is the most common cause of shoulder complaints and may lead to a plethora of problems, including biceps tendinitis (14). In fact, 95% of biceps tendinopathy patients have “shoulder impingement” as their primary diagnosis. (15) Because of common etiologies, biceps tendinopathy rarely occurs in isolation and over 90 percent co-exist with other impingement related pathologies of the shoulder such as rotator cuff tendinopathy/tears, labral tears, and shoulder instability (13,15,16). Additional risk factors for the development of biceps tendinopathy include repetitive shoulder flexion (lifting arm straight in front of you) or elbow bending, repetitive overhead activity, improper lifting technique, shoulder girdle muscle imbalances, poor posture, inflexibility, scapulothoracic or glenohumeral instability, repetitive overload, trauma, and osseous anatomical abnormalities that narrow the bicipital groove, including fracture, osteoarthritis, and congenital variations (17). Symptoms:
Patients with bicipital tendinopathy often complain of a deep throbbing ache over the anterior shoulder (4,18). Symptoms are often provoked by repetitive overhead activity (18,19). Symptoms increase when initiating activity (18). Nocturnal symptoms are common, particularly when sleeping on the affected shoulder (18,19). Patients often report mild relief from palliative measures, including heat, ice, stretching, and massage (18).
Tendon rupture:
Biceps tendons are one of the more common tendons to rupture. Tendon rupture is suggested by a history of a painful audible pop followed by relief. Risk factors associated with the biceps tendon rupture include chronic tendinopathy, concurrent rotator cuff tear, contralateral biceps tendon rupture, age over 40, poor conditioning, and the presence of a rheumatologic disease (19).Bruising & swelling with a visible bulge (Popeye deformity) where the muscle has retracted toward the elbow indicates tendon rupture. (19,58) Clinical evaluation of biceps tendinopathy will often demonstrate limited range of motion. Popping, catching, or locking movements during active range of motion testing may suggest a labral injury (20). Palpation should elicit the most characteristic finding of tenderness in the rotator interval and bicipital groove (1,21,22).
Do I need imaging?
Plain film (x-ray) imaging is of little value for the assessment of the biceps tendon but may identify osseous sources of impingement or other bony pathology. Ultrasound is a useful imaging technique for the biceps tendon (39-45). MRI may help identify ruptures of the long head of the biceps tendon or concurrent pathology, including rotator cuff lesions and labral tears (46,47). Overall, the evidence suggests that ultrasound and MRI are similar for assessing patients with suspected biceps abnormalities (74-76). Due to similar mechanisms of injury and indistinguishably blended anatomy, lesions of the bicep tendon are difficult to differentiate from rotator cuff pathology or labral tears (48). Biceps tendinopathy often co-exists with these and other pathologies of the shoulder (15,19,48).
What are the best treatment options for a biceps tendonopathy?
Conservative care is the most appropriate management for the majority of biceps tendinopathy patients (49).
The first phase of treatment is directed at pain relief and restoration of normal motion (51,52). Patients should limit activities that require repetitive overhead activity, elbow flexion, or forearm supination. Patients should specifically avoid military presses, upright rows, and wide-grip bench presses (52). Therapeutic modalities, including ice, heat, ultrasound, microcurrent, or e-stim may be appropriate to control symptoms as needed (52). The goal of rehab should be to establish a full, balanced, pain-free range of motion. (53)
Soft tissue techniques may include transverse friction massage or IASTM over the biceps tendon. Myofascial release and stretching exercises may be appropriate for the biceps, cervical spine, shoulder, and periscapular musculature.
Mobility exercises may include pendulum circumduction, wall walking, first phase of treatment should include early scapular stabilization exercises, via activation of the lower trapezius and serratus anterior. Examples of these exercises include YTWL and scapular protraction. As patient’s recover, strengthening may progress from isometric to concentric, then eccentric, and finally, sports specific rehab (51). Eccentric loading for the management of tendinopathies is a proven beneficial strategy and may be implemented as the patient recovers (51,54,71,72). Advanced strengthening exercises may include a bear hug, reverse fly, and resisted internal/external rotation at 90 degrees of abduction (52).
Limited cervicothoracic mobility, including a forward flexed posture, limits normal scapulohumeral rhythm and predisposes the shoulder to impingement-related disorders. There is evidence to suggest that cervicothoracic and thoracic spine manipulation is appropriate for patients with shoulder pain (33,55-57). Spinal manipulation may help decrease shoulder pain while improving mobility and function (33,55).
Medical management of biceps tendinopathy may include NSAIDs (66).
Ultrasound-guided, local anesthetic injection into the biceps tendon sheath may provide palliative relief for patients with primary biceps tendinitis, although injections directly into the tendon may increase the risk of rupture (59-63). Ultrasound guidance may produce up to a five-fold increase in pain relief versus non-ultrasound guided (64,65). Surgery is generally not considered for biceps tendinopathy unless prolonged (greater than three months) conservative measures have failed (66). Even in cases of tendon rupture, the value of surgery is questionable. Patients with complete rupture of the long head of the biceps tendon demonstrate 11-16% diminished strength in elbow flexion, forearm supination, and shoulder abduction. (67) Strength losses post-surgical repair range from 7-20 percent (67). Surgical repair (tenodesis) is usually reserved for younger individuals (<60), athletes, and manual workers (67-70).
At Creekside Chiropractic & Performance Center, we are highly trained to treat biceps tendonitis and tendonopathy. We are the only inter-disciplinary clinic in Sheboygan county that provides chiropractic, myofascial release, ART (Active Release Technique), massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiropractor by the Sheboygan Press.
Sources:
1. Patton WC, McCluskey GM III. Biceps tendinitis and subluxation. Clin Sports Med. 2001;20(3):505–529.
2. Longo UG, Loppini M, Marineo G, Khan WS, Maffulli N, Denaro V. Tendinopathy of the tendon of the long head of the biceps. Sports Med Arthrosc. Dec 2011;19(4):321-32.
3. Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. J Bone Joint Surg Br. Aug 2007;89(8):1001-9.
5. Moore K, Dalley A, Agur A, Clinically-oriented anatomy 6th edition Philadelphia, Pennsylvania, Lippincott Williams, and Wilkkins, 2010.
6. Clark JM, Harryman DT II. Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy. J Bone Joint Surg Am. 1992;74(5):713–725.
7. Habermeyer P, Walch G. The biceps tendon and rotator cuff disease. In: Burkhead WZ Jr, ed. Rotator Cuff Disorders. Philadelphia, Pa.: Lippincott Williams & Wilkins; 1996.
8. Cooper DE, Arnoczky SP, O'Brien SJ, Warren RF, DiCarlo E, Allen AA. Anatomy, histology, and vascularity of the glenoid labrum. An anatomical study. J Bone Joint Surg Am. 1992;74(1):46–52.
9. Curtis AS, Snyder SJ. Evaluation and treatment of biceps tendon pathology. Orthop Clin North Am. 1993;24(1):33–43.
10. Elser F, Braun S, Dewing CB, Giphart JE, Millett PJ. Anatomy, function, injuries, and treatment of the long head of the biceps brachii tendon. Arthroscopy. Apr 2011;27(4):581-92.
11. Bicos J. Biomechanics and anatomy of the proximal biceps tendon. Sports Med Arthrosc. Sep 2008;16(3):111-7.
12. Kibler WB. Scapular involvement in impingement: signs and symptoms. Instr Course Lect. 2006;55:35–43.
13. Churgay CA, Diagnosis and Treatment of Biceps Tendinitis and Tendinosis Am Fam Physician. 2009 Sep 1;80(5):470-476.
14. Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev 2003: CD004258.
15. Curtis AS, Snyder SJ. Evaluation and treatment of biceps tendon pathology. Orthop Clin North Am. Jan 1993;24(1):33-43. http://reference.medscape.com/...
16. Abrams JS. Special shoulder problems in the throwing athlete: pathology, diagnosis, and nonoperative management. Clin Sports Med. 1991;10(4):839–861.
17. Gonzalez P, Biceps Tendinopathy Clinical Presentation http://emedicine.medscape.com/... accessed 15 March 2014.
18. Larson HM, O'Connor FG, Nirschl RP. Shoulder pain: the role of diagnostic injections. Am Fam Physician. Apr 1996;53(5):1637-47
19. Harwood MI, Smith CT. Superior labrum, anterior-posterior lesions and biceps injuries: diagnostic and treatment considerations. Prim Care. 2004;31(4):831–855.
20. Sethi N, Wright R, Yamaguchi K. Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg. 1999;8(6):644–654.
21. House J, Mooradian A. Evaluation and management of shoulder pain in primary care clinics. South Med J. 2010;103(11):1129-35;
22. Nho SJ, Strauss EJ, Lenart BA, et al. Long head of the biceps tendinopathy: diagnosis and management. J Am Acad Orthop Surg. 2010;18(11):645-656.
23. Kibler BW, Sciascia AD, Hester P, Dome D, Jacobs C. Clinical utility of traditional and new tests in the diagnosis of biceps tendon injuries and superior labrum anterior and posterior lesions in the shoulder. Am J Sports Med. 2009 Sep;37(9):1840-7.
24. Hultby R, Razmjouh, Accuracy of the speeds and Yergason’s tests in detecting biceps pathology. Arthroscopy, 2004, Mar; 20 (3): 231-6.
25. Harwood MI, Smith CT. Superior labrum, anterior-posterior lesions and biceps injuries: diagnostic and treatment considerations. Prim Care. 2004;31(4):831–855.
26. Berg D, Worzala K, eds. Atlas of Adult Physical Diagnosis. Philadelphia, Pa.: Lippincott Williams & Wilkins; 2005:240.
28. McFarland EG. Examination of the Shoulder: The Complete Guide. 2006 Thieme Medical Publishers Inc. p 229
29. Neer CS II. Impingement lesions. Clin Orthop Relat Res. 1983;(173):70–77.
30. Greene W, Griffin LY, eds. Special tests for the shoulder. In: Essentials of Musculoskeletal Care. 3rd ed. Rosemont, Ill.: American Academy of Orthopaedic Surgeons; 2005:154–155.
31. Speed CA. Fortnightly review: Corticosteroid injections in tendon lesions. BMJ. 2001;323(7309):382–386.
32. Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional Interdependence: A Musculoskeletal Examination Model Whose Time Has Come. J Ortho Sports Phys Ther. 2007; 37(11): 658-660.
33. Crosbie J, Kilbreathe SL, Hooman L, York S. Scapulohumeral rhythm and associated spinal motion. Clin Biomechan. 2008; 23: 184-192.
34. Laudner KG, Myers JB, Pasquale MR, Bradley JP, Lephart SM. Scapular dysfunction in throwers with pathologic internal impingement. Journal of Orthopaedic and Sports Physical Therapy. 2006;36(7):485–494.
35. Kibler WB. Scapular involvement in impingement: signs and symptoms. Instr Course Lect. 2006;55:35–43.
36. Abrams JS. Special shoulder problems in the throwing athlete: pathology, diagnosis, and nonoperative management. Clin Sports Med. 1991;10(4):839–861.
37. Fisk C. Adaptation of the technique for radiography of the bicipital groove. Radiol Technol. Sep 1965;37:47-50.
39. Pfahler M, Branner S, Refior HJ. The role of the bicipital groove in tendopathy of the long biceps tendon. J Shoulder Elbow Surg. 1999;8(5):419–424.
40. Iagnocco A, Filippucci E, Meenagh G, et al. Ultrasound imaging for the rheumatologist. I. Ultrasonography of the shoulder. Clin Exp Rheumatol. 2006;24(1):6–11.
41. Martinoli C, Bianchi S, Prato N, et al. US of the shoulder: non-rotator cuff disorders. Radiographics. 2003;23(2):381–401.
42. O'Connor PJ, Rankine J, Gibbon WW, Richardson A, Winter F, Miller JH. Interobserver variation in sonography of the painful shoulder. J Clin Ultrasound. 2005;33(2):53–56.
43. Lecoq B, Levasseur R, Fournier L, Schmutz G, Marcelli C. Atypical pattern of acute severe shoulder pain: contribution of sonography. Joint Bone Spine. 2004;71(6):592–594.
44. King LJ, Healy JC. Imaging of the painful shoulder. Man Ther. 1999;4(1):11–18.
45. Middleton WD, Reinus WR, Totty WG, Melson GL, Murphy WA. US of the biceps tendon apparatus. Radiology. 1985;157(1):211–215.
46. Armstrong A, Teefey SA, Wu T, et al. The efficacy of ultrasound in the diagnosis of long head of the biceps tendon pathology. J Shoulder Elbow Surg. Jan-Feb 2006;15(1):7-11.
47. Smith DL, Campbell SM. Painful shoulder syndromes: diagnosis and management. J Gen Intern Med. May-Jun 1992;7(3):328-39
48. Harwood MI, Smith CT. Superior labrum, anterior-posterior lesions and biceps injuries: diagnostic and treatment considerations. Prim Care. 2004;31(4):831–855.
49. Ryu JH, Pedowitz RA. Rehabilitation of biceps tendon disorders in athletes. Clin Sports Med. 2010;29(2):229-46, vii-viii.
50. Bennett WF. Specificity of the Speed's test: arthroscopic technique for evaluating the biceps tendon at the level of the bicipital groove. Arthroscopy. 1998;14(8):789-796.
51. Rees JD, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology (Oxford). May 2006;45(5):508-21.
52. Krupp RJ, Kevern MA, Gaines MD, Kotara S, Singleton SB. Long head of the biceps tendon pain: Differential diagnosis and treatment. J Orthop Sports Phys Ther. 2009;39(2):55-70. doi: 10.2519/jospt.2009.2802.
53. Abrams JS. Special shoulder problems in the throwing athlete: pathology, diagnosis, and nonoperative management. Clin Sports Med. 1991;10(4):839–861.
54. Boone JK, Dee AE, Gildea CP, Kavanaugh CR, Moore SD, Quinlevan ME, Reichard RL, Ronan KA, Sanchez Z, Whittington AG. Eccentric Training. University of Kentucky, AT 690, Spring 2011
55. Strunce JB, et al. The Immediate Effects of Thoracic Spine and Rib Manipulation on Subjects with Primary Complaints of Shoulder Pain J Man Manip Ther. 2009; 17(4): 230–236.
56. Walser RF, Meseve BB, Boucher TR. The Effectiveness of Thoracic Spine Manipulation for the Management of Musculoskeletal Conditions: A Systematice Review and Meta-Analysis of Randomized Controlled Trials. J Man Manip Ther. 2009; 17(4): 237-246.
57. Muth S et al. The Effects of Thoracic Spine Manipulation in Subjects With Signs of Rotator Cuff Tendinopathy Journal of Orthopaedic & Sports Physical Therapy, 2012, Volume: 42 Issue: 12 Pages: 1005-1016
58. Gill HS, Rassi GE, Bahk MS, Castillo RC, McFarland EG. Physical examination for partial tears of the tendon. Am J Sports Med. 2007;3(8):1334–40.
59. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59–63.
60. Kapetanos G. The effect of the local corticosteroids on the healing and biomechanical properties of the partially injured tendon. Clin Orthop Relat Res. 1982;(163):170–179.
61. Fredberg U. Local corticosteroid injection in sport: review of literature and guidelines for treatment. Scand J Med Sci Sports. 1997;7(3):131–139.
62. Pfenninger JL. Joint and soft tissue aspiration and injection. In: Pfenninger JL, FowlerGC, eds. Procedures for Primary Care Physicians. Philadelphia, Pa.: Saunders; 1994:1036–1054.
63. Lee PN, Lee M, Haq AM, Longton EB, Wright V. Periarthritis of the shoulder. Trial of treatments investigated by multivariate analysis. Ann Rheum Dis. 1974;33(2):116–119.
64. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308–314.
65. Sofka CM, Collins AJ, Adler RS. Use of ultrasonographic guidance in interventional musculoskeletal procedures: a review from a single institution. J Ultrasound Med. 2001;20(1):21–26.
66. Ahrens PM, Boileau P. The long head of biceps and associated tendinopathy. J Bone Joint Surg Br. 2007;89(8):1001–1009.
67. Sturzenegger M, Béguin D, Grünig B, Jakob RP. Muscular strength after rupture of the long head of the biceps. Arch Orthop Trauma Surg. 1986;105(1):18-23.
68. Mariani EM, Cofield RH, Askew LJ, Li GP, Chao EY. Rupture of the tendon of the long head of the biceps brachii. Surgical versus nonsurgical treatment. Clin Orthop Relat Res. 1988;(228):233–239.
69. Froimson AI. O I. Keyhole tenodesis of biceps origin at the shoulder Clin Orthop Relat Res. 1975;(112):245–249.
70. Mariani EM, Cofield RH, Askew LJ, Li GP, Chao EY. Rupture of the tendon of the long head of the biceps brachii. Surgical versus nonsurgical treatment. Clin Orthop Relat Res. 1988;(228):233–239.
71. Stanish W, Curwin S, Mandell S. Tendonopathy: Its etiology and treatment. Oxford, England: University Press; 2000.
72. Stanish WD, Rubinovich RM, Curwin S. Eccentric exercise in chronic tendonopathy. Clin Orthop Relat Res. Jul 1986(208):65-68.
73. Borms D, et al. Biceps Disorder Rehabilitation for the Athlete: A Continuum of Moderate- to High-Load Exercises. The American Journal of Sports Medicine. Vol 45, Issue 3, pp. 642 – 650
74. Skendzel JG, Jacobson JA, Carpenter JE, Miller BS. Long head of biceps brachii tendon evaluation: accuracy of preoperative ultrasound. AJR 2011; 197:942–948
75. Petchprapa CN, Beltran LS, Jazrawi LM, Kwon YW, Babb JS, Recht MP. The rotator interval: a review of anatomy, function, and normal and abnormal MRI appearance. AJR 2010; 195:567–576
76. Tuite MJ, et al. Imaging Evaluation of Nonacute Shoulder Pain. AJR Am J Roentgenol. 2017 May 24:1-9. doi: 10.2214/AJR.17.18085. [Epub ahead of print]