
TMJ Dysfunction
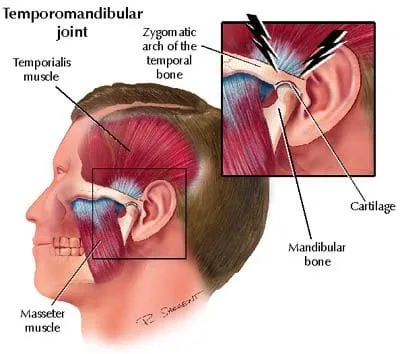
Temporomandibular Joint Disorder (TMJ Dysfunction) describes a complex group of muscle and joint disorders affecting the TMJ, leading to pain, dysfunction and eventually degeneration. Most causes of TMJ dysfunction can be divided into either muscular or arthrogenous (joint).
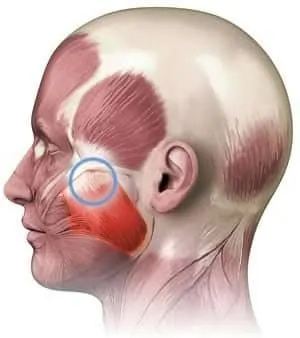
TMJ dysfunction of muscle origin is more common (1) and may arise from: muscular hypertonicity, trigger points, fascial restrictions and/or functional muscle imbalance of the muscles used for chewing. One of the most commonly involved muscles is the masseter. Other recognized triggers for muscular TMJ dysfunction include: bruxism, clenching, neck joint dysfunction (2), postural syndromes, especially a forward head posture (3,4), and trauma (5). TMJ dysfunction symptoms may occur in up to one third of those patients involved in a whiplash injury (6). Psychosocial disturbances including stress and depression, are another widely recognized co-morbidity for TMJ dysfunction.
I heard jaw problems are because of having my teeth pulled?
Studies vary on the relationship of premolar extraction (tooth pulling) to the development of TMJ dysfunction, but recent evidence shows that tooth pulling is not related to jaw dysfunction. (7).
How common is TMJ Dysfunction?
Estimates for the incidence of TMJ dysfunction vary between 4-25% (8,9). Up to 3% of Americans seek treatment for TMJ related issues each year (21). At presentation, most patients are 20-50 years old and prevalence is 2-3 times higher in females.
What are the symptoms of TMJ Dysfunction?
Typical symptoms include: clicking, restricted opening, transient locking and pain. Symptoms may be worsened by chewing. TMJ pain is generally described as an “ache” just in front of the ear canal but may refer to other areas of the face, head, neck and shoulders (6). TMJ dysfunction patients often suffer concurrently from headaches, suggesting a common link arising from the upper cervical spine (10).
Do I need imaging for TMJ Dysfunction?
Often times, a trial of care of 4-6 weeks including treatment will proceed any imaging. If imaging is needed, CT is the imaging of choice (over 4 times better than plain films) for identifying TMJ osteoarthritis. The reliability of MRI is also excellent for detecting disc displacements and effusion (12). Diagnostic ultrasound is a non-invasive imaging option that can easily identify TMJ disc displacement.
Treatment options for TMJ Dysfunction:
Management should be conservative and simple, focusing on three main points: manual therapies, exercise and avoidance of aggravating activities.
Manual therapy is an effective treatment for TMJ Dysfunction. (30) In fact, non-surgical intervention for myogenous TMJ has been shown to be as effective as any surgical intervention (13). TMJ non-thrust mobilization is often indicated (10).Manipulation of the cerviocranial, cervical and thoracic spine may be necessary (16). Chiropractic cervical spine manipulation has been shown to increase maximal bite force (31).
Exercises to improve posture and TMJ function have been shown to be beneficial (10,17,18). Stretching exercises should address tightness in the masseter, SCM, levator and suboccipitals. Patient’s should also work on chin retractions, deep neck flexion and chin depression exercises.
Patients should avoid aggravating activities like chewing gum or eating "rubbery" type foods. Patients should also limit unnecessary talking (18,19). Glucosamine and chondroitin sulfate have shown success in managing TMJ dysufuction (34). Supplementation with bromelin or MSM may also be beneficial. A custom fitted mouth guard can help prevent clenching and promote relaxation of muscles (20). Patients with symptoms at night should avoid stressful activity before bedtime and be aware of their sleeping position.
At Creekside Chiropractic & Performance Center, we are highly trained to treat this condition. We are the only inter-disciplinary clinic in Sheboygan county that provides chiropractic, myofascial release, ART (Active Release Technique), dry needling, massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiropractor in Sheboygan by the Sheboygan Press ('19,'20,'21).
Evidence Based-Patient Centered-Outcome Focused
Sources:
1. Lane, N. Osteoarthritis of the Hip. NEJM 357;14, Oct 4, 2007
2. Byrd J. Evaluation of the hip: history and physical examination. North American Journal Of Sports Physical Therapy: NAJSPT [serial online]. November 2007;2(4):231-240.
3. Khan, A.M., McLoughlin, E. Hip Osteoarthritis: Where is the Pain? Ann R Coll Surg Engl. 2004 March 86(2) 119-121
4. Bird P, Oakley S, ShnierR, Kirkham B. Prospective evaluation of magnetic resonance imaging and physical examination findings in patients with greater trochantericpain syndrome. Arthritis And Rheumatism [serial online]. September 2001;44(9):2138-2145.
5. Martin RL, IrrgangJJ, SekiyaJK. The diagnostic accuracy of a clinical examination in determining intra-articularhip pain for potential hip arthroscopy candidates. Arthroscopy. 2008;38:542-550.
6. SutliveT, Lopez H, Childs J, et al. Development of a clinical prediction rule for diagnosing hip osteoarthritis in individuals with unilateral hip pain. Journal Of Orthopaedic& Sports Physical Therapy [serial online]. September 2008;38(9):542-550.
7. SuenagaE, Noguchi Y, Iwamoto Y, et al. Relationship between the maximum flexion-internal rotation test and the torn acetabularlabrum of a dysplastic hip. Journal Of OrthopaedicScience: Official Journal Of The Japanese OrthopaedicAssociation [serial online]. 2002;7(1):26-32.
8. Martin RL, IrrgangJJ, SekiyaJK. The diagnostic accuracy of a clinical examination in determining intra-articularhip pain for potential hip arthroscopy candidates. Arthroscopy. 2008;38:542-550.
9. Narvani A, TsiridisE, Kendall S, ChaudhuriR, Thomas P. A preliminary report on prevalence of acetabularlabrum tears in sports patients with groin pain. Knee Surgery, Sports Traumatology, Arthroscopy [serial online]. November 2003;11(6):403-408.
10. Lesher, J., Dreyfuss, P., Hager, N. Hip Joint Pain Referral Patterns: A Descriptive Study. Pain Medicine Vol. 9(1), 2008
11. DeAngelis, Nicola A. MD; Busconi, Brian D. MD Assessment and Differential Diagnosis of the Painful Hip. Clinical Orthopedics. Volume 406, January 2003, pp 11-18
12. Margo, K., Drezner, J., Motzkin, D. Evaluation and Management of Hip Pain: An Alogrithmic Approach Journal of Family Parctice Vol 52(8) August 2003
13. Stener-Victorin E, Kruse-Smidje C, Jung K. Comparison between
electro-acupuncture and hydrotherapy, both in combination with patient
education and patient education alone, on the symptomatic treatment
of osteoarthritis of the hip. Clin J Pain 2004;20:179–85.
14. Cochrane T, Davey RC, Mattes Edwards SM. Randomised controlled
trial of the cost-effectiveness of water based therapy for lower limb
osteoarthritis. Health Tech Assess 2005;9:1–114.
15. Altman R, Alarcon G, Appelrouth D, Bloch D, Borenstein D, Brandt K, et al. The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum 1991;34:505–14.
16. Brantingham J, Williams A, Parkin-Smith G, Weston P, Wood T. A controlled, prospective pilot study into the possible effects of chiropractic manipulation in the treatment of osteoarthritis of the hip. Euro J Chiropr. 2003;51:149-166.
17. Hoskins W, McHardy A, Pollard H, Windsham R, Onley R. Chiropractic treatment of lower- extremity conditions: a literature review. J Manipulative Physiol Ther. Oct 2006;29(8):658- 671.
18. Brantingham JW, Bonnefin D, Perle SM, et al. Manipulative therapy for lower-extremity conditions: update of a literature review. J Manipulative Physiol Ther. Feb 2012;35(2):127- 66.(2):127-166.
19. MacDonald C, Whitman J, Cleland J, Smith M, Hoeksma H. Clinical outcomes following manual physical therapy and exercise for hip osteoarthritis: A case series. J Orthop Sports Phys Ther. Aug 2006;36(8):588-599.
20. Brantingham JW, Globe G, Cassa T, et al. A single-group pre-test post-test design using full kinetic chain manipulative therapy with rehabilitation in the treatment of 18 patients with hip osteoarthritis. J Manipulative Physiol Ther. July/August 2010;33(6):445-457.
21. Brantingham JW, Globe G, Cassa T, et al. A single-group pre-test post-test design using full kinetic chain manipulative therapy with rehabilitation in the treatment of 27 patients with hip osteoarthritis J Amer Chiropr Assoc. August 2010;47(6):8-26.
22. de Luca K, Pollard H, Brantingham J, Globe G, Cassa T. Chiropractic management of the kinetic chain for the treatment of hip osteoarthritis: an Australian case series. J Manipulative Physiol Ther. Jul-Aug 2010;33(6):474-479.
23. Brantingham JW, Parkin Smith, Cassa T, et al. Full kinetic chain manual and manipulative therapy plus exercise compared with targeted manual and manipulative therapy plus exercise for symptomatic osteoarthritis of the hip - a randomized controlled trial. Arch Phys Med Rehabil. 2012 93(2):259-267.
24. Abbott JH, Robertson MC, Chapple C, et al. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: a randomized controlled trial. 1: clinical effectiveness. Osteoarthritis and Cartilage 2013;21(4):525-534.
25. Zhang W, Moskowitz R, Nuki G, et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidence-based, expert consensus guidelines. Osteoarthritis and Cartilage. 2008;16:137-162.
26. Poulsen E, Hartvigsen J, Christensen HW, Roos EM, Vach W, Overgaard S. Patient education with or without manual therapy compared to a control group in patients with osteoarthritis of the hip. A proof-of-principle three-arm parallel group randomized clinical trial. Osteoarthritis Cartilage. Oct 2013;21(10):1494-1503.
27. French HP, Cusack T, Brennan A, et al. Exercise and manual physiotherapy arthritis research trial (EMPART) for osteoarthritis of the hip: a multicenter randomized controlled trial. Archives of Physical Medicine and Rehabilitation. Feb 2013;94(2):302-314.
28. Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis Care & Research. Apr 2012;64(4):465-474.
29. de Luca K, Pollard H, Brantingham J, Globe G, Cassa T. A randomized controlled trial of chiropractic management of the lower limb kinetic chain for the treatment of hip osteoarthritis: a study protocol J Chiro Med. 2011;10(2):86-92.
30. Official Disability Guidelines. The11th edition of the ODG for Treatment in Workers Compensation (updated 7/3/2013). Hip Osteoarthritis. www.worklossdatainstitute.verioiponly.com/.
31. Moseley JB, Jr., Wray NP, Kuykendall D, Willis K, Landon G. Arthroscopic treatment of osteoarthritis of the knee: a prospective, randomized, placebo-controlled trial. Results of a pilot study. The American Journal of Sports Medicine. Jan-Feb 1996;24(1):28-34.
32. Moseley J, O’Malley K, Petersen N, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002;347(2):81-88.
33. Nutton RW. Is arthroscopic surgery a beneficial treatment for knee osteoarthritis? Nat Clin Pract Rheumatol. Mar 2009;5(3):122-123.
34. Laupattarakasem W, Laopaiboon M, Laupattarakasem P, Sumananont C. Arthroscopic debridement for knee osteoarthritis. Cochrane Database Syst Rev. 2008(1):CD005118.
35. Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. Sep 11 2008;359(11):1097-1107.
36. Zhang W, Nuki G, Moskowitz RW, et al. OARSI recommendations for the management of hip and knee osteoarthritis: part III: Changes in evidence following systematic cumulative update of research published through January 2009. Osteoarthritis Cartilage. Apr 2010;18(4):476-499.
37. Pollard H, Ward G. A study of two stretching techniques for improving hip flexion range of motion. J of Manip & Physiol Ther. Sep 1997;20(7):443-447.
38. V aux P . Hip osteoarthritis: a chiropractic approach. Euro J Chiropr 1998;46(1):17-22.
39. Vaarbakken K, Ljunggren AE. Superior effect of forceful compared with standard traction
mobilizations in hip disability? Adv Physiother. Sep 2007;9(3):117-128.
40. Fransen M, McConnell S, Hernandez-Molina G, Reichenbach S. Does land-based exercise reduce pain and disability associated with hip osteoarthritis? A meta-analysis of randomized controlled trials. Osteoarthritis Cartilage. May 2010;18(5):613-620.
41. Hoeksma HL, Dekker J, Ronday HK, et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: A randomized clinical trial. Arthritis Rheum. Oct 15 2004;51(5):722-729.
42. Official Disability Guidelines. The11th edition of the ODG for Treatment in Workers Compensation (updated 7/3/2013). General Information. Patricia Whelan, Publisher.
43. Sampath KK, Mani R, Miyamori T, Tumilty S. The effects of manual therapy or exercise therapy or both in people with hip osteoarthritis: a systematic review and
metaanalysis.. Clin Rehabil. 2016 Dec;30(12):1141-1155.