

Achilles Tendon Pain
Achilles Tendonitis, Tendonopathy
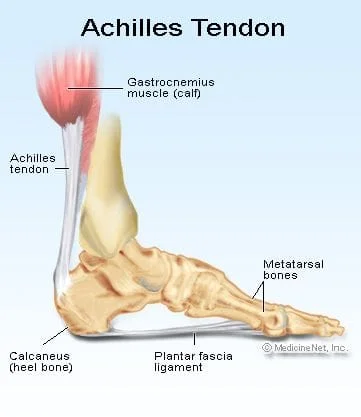
Did you know that the achilles tendon is the strongest and largest tendon in the human body? This isn't by accident, as it has to transmit a lot of force through foot, ankle, and leg. It is constantly under intense pressure, as exercises such as running continually places up to pressure up to 12.5 times your body weight each step.
The Achilles tendon may be acutely strained or ruptured due to an excessive stretch or force. Strains occur when the collagen fibers are stretched by more than 4%. Ruptures occur when stretch exceeds 8% (4,5).
Unlike acute injuries that cause inflammation, tendinopathy is characterized by repeated overloading, microtearing, failed healing, and subsequent tendon degeneration (3,4,6,7). The process begins with collagen fiber disruption and ends in a disorganized healing process that fails to regenerate a “normal” tendon. Failed healing is blamed on an ineffective microvascular system (8,9).
I have flat feet, does that affect the achilles tendon?
Hyperpronation stresses the medial attachment of the Achilles tendon (10).
Does the achilles tendon have any blood supply?
Contrary to popular belief, it does! Although, there is what is called a "watershed area", which is 2-6cm above the heel. This area has very little blood flow, has a smaller tendon cross section, and is subject to repetitive excess motion. This is the most common site for degeneration and rupture (12,13).
How common are achilles tendon injuries?
Achilles tendon injuries affect between 250,000 and 1 million people per year in the United States (14,15). Most are middle-aged males 30's to 40's (14,16). Interestingly, Achilles tendon injuries occur more frequently on the left side (16). Patients who have had a previous achilles tendon rupture are at significantly higher risk for tendon rupture on the other side (17).
Who is most likely to have an achilles injury?
Two-thirds of all Achilles tendon injuries involve athletes. (18) Runners are up to 10 times more likely to suffer Achilles tendon injuries (18). The Athletes are at greater risk during speed training or sprinting (19). Runners who assume a midfoot or forefoot strike pattern (rather than heel strike) may be at even greater risk of injury (20). Not surprisingly, a higher risk has been identified in other sports that involve running or jumping. The most likely sports to produce an Achilles tendinopathy: running (53%), soccer (11%), dance (9%), gymnastics (5%), racquet sports (2%), football (1%) (14,21).
Are there risk factors for achilles injury?
Risk factors for Achilles injury include improper warm up, overtraining, running on hard surfaces, excessive stair or hill climbing, improper arch support/ footwear, poor conditioning, and abruptly starting activity after a period of inactivity (19,22-26). Wearing high-heeled shoes may lead to shortening of the calf muscles, predisposing women to Achilles tendinopathy (27). Intrinsic factors include over pronation , flat feet, calf inflexibility or weakness, limited ankle dorsiflexion, and limited subtalar joint motion (14,22-26). Systemic risk factors include diabetes, hypertension, inflammatory arthritis scubas psoriatic arthritis or rheumatoid arthritis, gout, obesity, and the use of corticosteroids or quinolones (broad spectrum antibiotics) (28,81,84).
What does an achilles tendonitis feel like?
Complaints include pain or tenderness in the tendon or heel that intensifies with activity, especially walking or running. Patients may report difficulty when attempting to stand on their toes or walking steps- particularly down stairs. Morning pain and stiffness are common. Patients may report warmth and swelling that increases throughout the day, related to activity.
Is my big toe somehow connected to this injury?
Limited hallux motion (your big toe) has been associated with Achilles tendon pain (33). This can be assessed by inspecting the inside of your shoe. If there is a lack of wear on the first toe with lots of wear on toes 2-5, you may not be utilizing your big toe properly during the push off phase of your gait.
Do I need X-rays for achilles pain?
Radiographs are often unnecessary for the diagnosis of Achilles tendinopathy (35). Ultrasound may be an efficient cost-effective means of evaluating the Achilles tendon (39). Ultrasound or MRI may help identify and define tendon pathology.
What are the treatment options for achilles tendonitis and pain?
Nonoperative treatment is the most common treatment for Achilles tendinopathy (81).
What about ice or heat and ibuprofen for achilles pain?
“Traditional” treatment plans based solely on rest, therapy modalities, orthotics, and NSAIDs have failed to demonstrate benefit for Achilles tendinopathy patients (41). Passive modalities including ice, ultrasound, electrical stimulation, and low-level laser also lack support (42).
What is the current standard for achilles tendonitis pain treatment?
The current standard of care for Achilles tendinopathy includes a combination of rest, eccentric rehabilitation, and correction of mechanical faults through manual therapy and other treatments. Studies have demonstrated excellent results in up to 85% of patients undergoing appropriate conservative care. (43) Initially, patients may need to limit or stop activities that cause pain. Significant strains may require the use of crutches or a boot. Runners may need to switch to swimming, cycling, or other activities that limit stress to the Achilles tendon. Patients should avoid shoes with an excessively rigid heel tab to reduce irritation.
Eccentric exercise programs are effective for treating Achilles tendinopathy. (41,44-54) Eccentric training is more effective than concentric training for reducing pain and improving function (52,55). In fact, research suggests that eccentric strength training programs are more than twice as effective as concentric programs for the treatment of Achilles tendinopathy (52).
What is the best rehab exercise for achilles tendonopathy?
A proven program by Alfredson (45) incorporates single leg eccentric heel drops off the edge of a step. Heel drops should be performed with the knee both straight and bent, three sets of 15 repetitions, twice per day for 12 weeks. Heel drops should occur slowly on a 4-10 second count. (56). The patient should use the non-injured leg to return to the “heel up” start position, thereby avoiding concentric contractions. Moderate pain during this exercise is acceptable but if pain is excessive, the patient should assist downward motion with the non-injured leg.
How do I know if I am doing enough or too much exercise?
Increases in night pain indicate the current rehab load is excessive. Progression advances when the patient tolerates a given level of tensile load. (92).
What are the best manual therapies for achilles tendonopathy?
Soft tissue manipulation, stretching, and myofascial release techniques are necessary to promote flexibility of the calf muscles. IASTM can be used to release adhesions within the Achilles tendon. As an additional benefit, IASTM may accelerate healing, possibly via controlled microtrauma (57,78-80). Manipulation may be necessary to eliminate restrictions in the kinetic chain, particularly within the ankle (58). Clinicians may consider the use of a 7-15 mm heel lift (bilaterally) to minimize dorsiflexion stress. Arch supports or orthotics may be necessary to correct hyperpronation (76).
How can I go about increasing my training?
Athletes should introduce new activities slowly and avoid increasing activity, particularly running, by more than 10% per week. Runners should begin on smooth, shock-absorbent surfaces and start out at a lower intensity and distance- first increasing distance, then pace. Athletes should avoid training on hard or un-level surfaces, including hills.
What are the return to play guidelines for the achilles tendon?
Return-to-play criteria for Achilles tendon strains or ruptures include the “Triple 5” (60):
1. Ankle dorsiflexion is within 5 degrees of the uninjured side,
2. Calf circumference (measured 10 cm distal to the tibial tuberosity) is within 5 mm of the uninjured side
3. The patient is able to perform 5 sets of 25 single leg heel raises
What about other treatment options?
Patients who fail a trial of conservative care should be referred, but proven alternatives are scarce. Medical co-management is of limited benefit in this case. NSAIDs may relieve symptoms but have little long-term effect on outcome (61,62).
What about cortisone injections?
Cortisone injections are unproven for the treatment of Achilles tendinopathy and carry a possible increased risk of tendon rupture (63,64).
What about shockwave therapy or PRP injections?
Extracorporeal shock-wave therapy (ESWT) or platelet-rich plasma (PRP) injections are controversial alternatives. (65-68) ESWT (originally developed as lithotripsy) is thought to break up calcific deposits and stimulate fibroblast activity to encourage healing and may be appropriate for Achilles tendinopathy. (81,82,91). PRP treatments consist of injecting platelet-rich plasma into a tendon to create a concentrated trigger of growth factors and chemoattractants for macrophages and fibroblasts, which gradually repair the damaged collagen. (69) Some clinicians suggest benefit from PRP injections, but others refute its usefulness for Achilles tendinopathy (81,83).
What if I have a achilles tendon rupture? Do I need surgery?
Surgical management is often considered for Achilles tendon ruptures, although several studies, including at least one randomized clinical trial, suggests at least equivalent results between surgical and conservative management (59,71,72,85)
At Creekside Chiropractic & Performance Center, we are highly trained to treat this condition. We are the only inter-disciplinary clinic providing services to Sheboygan, Sheboygan Falls, Plymouth, and Oostburg including chiropractic, manual therapy, myofascial release, ART (Active Release Technique), massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiroractor in Sheboygan by the Sheboygan Press.
Evidence Based-Patient Centered-Outcome Focused
Sources:
1. O’Brien, M. Functional anatomy and physiology of tendons (1992) Clinical Sports Medicine 11:505-20
2. Komi PV, Fukashiro S, Jarvinen M. Biomechanical loading of Achilles tendon during normal locomotion. Clin Sports Med 1992;11: 521–31.
3. Gibbon, W.W., Cooper, J.R., Radcliffe, G.S. (1999). Sonographic incidence of tendon microtears in athletes with chronic Achilles tendinosis. British Journal of Sports Medicine 33, 129–30.
4. Kvist M. Achilles tendon injuries in athletes. Sports Med1994;18:173–201.
5. Leppilahti JOS, Karpakka J, et al. Overuse injuries of the Achilles tendon. Ann Chir Gynaecol 1991;80: 202–7.
6. Kader, D., Saxena, A, Movin, T, and Maffulli, N. (2002) Achilles tendinopathy: some aspects of basic science and clinical management. British Journal of Sports Medicine 36, 239-249.
7. Astrom M. On the nature and etiology of chronic achilles tendinopathy. PhD thesis, Lund University, Sweden, 1997.
8. Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). J Bone & Jt. Surg 1999. 81-A(2):259-278.
9. Leadbetter WB. Cell-matrix response in tendon injury. Clin Sports Med 1992;11(3):568-569
10. Footlogics. Lower Limb Biomechanics www.footlogics.co/ lower –limb-biomechanics.html. accessed 1/2/14
11. Wren TAL, Lindsey DP, Beaupré GS, Carter DR. Effects of creep and cyclic loading on the mechanical properties and failure of human Achilles tendons. Ann Biom Engineering. 2003;31:710–717.
12. Jacobs BA. Achilles Tendon Rupture. emedicine. medscape.com accessed 1/2/14
13. Chen, Tony M.; Rozen, Warren M.; Pan, Wei-ren; Ashton, Mark W.; Richardson, Martin D.; Taylor, G. Ian. (2009) The arterial anatomy of the Achilles tendon: Anatomical study and clinical implications Clinical Anatomy vol. 22 issue 3, 377–385.
14. Gebauer M, Beil FT, Beckmann J, Sárváry AM, Ueblacker P, Ruecker AH. et al. Mechanical evaluation of different techniques for Achilles tendon repair. Arch Orthop Trauma Surg. 2007;127:795–799.
15. Lauer, Harvey. American Sports Data, Inc. A Comprehensive Study of Sports Injuries in the U.S., 2003.
16. Suchak AA, Bostick G, Reid D, Blitz S, Jomha N. The incidence of Achilles tendon ruptures in Edmonton, Canada. Foot and Ankle International 2005;26(11):932-936.
17. Aroen A, Helgo D, Granlund OG, Bahr R. Scand J Med Sci Sports. 2004 Feb;14(1):30-3.
18. Rolf CMT. Etiology, histopathology, and outcome of surgery in achillodynia. Foot Ankle Int 1997;18: 565–9.
19. Clement, D.B., Taunton, J.E., Smart, G.W. (1984). Achilles tendinitis and peritendinitis: Etiology and treatment. American Journal of Sports Medicine 12, 179–84.
20. Almonroeder T, Willson JD, Kernozek TW. The effect of foot strike pattern on achilles tendon load during running. Ann Biomed Eng 2013 May 3.
21. Kvist M. Achilles tendon overuse injuries. PhD thesis, University of Turku, Finland, 1991.
22. Asplund CA, Best TM. Achilles tendon disorders. BMJ. Mar 12 2013;346:f1262.
23. Keene JS. Tendon injuries of the foot and ankle. In: DeLee JC, Drez D, eds. Orthopaedic Sports Medicine. Philadelphia, Pa: WB Saunders; 1994:1788-94.
24. Albers D, Hoke B. Techniques in Achilles tendon rehabilitation. Tech Foot Ankle Surg. 2003;2(3):208-19.
25. Saltzman C, Bonar S. Tendon problems of the foot and ankle. In: Lutter LD, Mizel MS, Pfeffer GB, eds.Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, Ill: American Academy of Orthopaedic Surgeons; 1994:236-73.
26. Albers D, Hoke B. Techniques in Achilles tendon rehabilitation. Tech Foot Ankle Surg. 2003;2(3):208-19.
27. Csapo, R., Maganaris, C.N., Seynnes, O.R., Narici, M.V. (2010) On Muscle, Tendon and High Heels. Journal of Experimental Biology 213 3582- 2588.
28. van der Linden, Paul D.; Sturkenboom, Miriam C. J. M.; Herings, Ron M. C.; Leufkens, Hubert M. G.; Rowlands, Sam; Stricker, Bruno H. Ch. (2003) Increased Risk of Achilles Tendon Rupture With Quinolone Antibacterial Use, Especially in Elderly Patients Taking Oral Corticosteroids JAMA Internal Medicine vol 163 no.15.
29. Robinson JM, Cook JL, Purdam C, Visentini PJ, Ross J, Maffulli N, Taunton JE, Khan KM; Victorian Institute Of Sport Tendon Study Group. Br J Sports Med. 2001 Oct;35(5):335-41.
30. Maffulli N. The clinical diagnosis of subcutaneous tear of the Achilles tendon. A prospective study in 174 patients. Am J Sports Med 1998. 26266–270.270.
31. Hein T, Janssen P, Wagner-Fritz U, et al. Prospective analysis of intrinsic and extrinsic risk factors on the development of Achilles tendon pain in runners. Scand J Med Sci Sports 2013 October 31
32. Nadler SF, Malanga GA, DePrince M, et al. The relationship between lower extremity injury, low back pain, and hip muscle strength in male and female collegiate athletes. Clin J Sport Med 2000;10(2):89-97.
33. Payne C, Chuter V, Miller K. Sensitivity and specificity of the functional hallux limitus test to predict foot function. J Am Podiatr Med Assoc 2002;92(5):269-271.
34. Van Gheluwe B, Dananberg HJ, Hagman F, Vanstaen K. Effects of hallux limitus on plantar foot pressure and foot kinematics during walking. J Am Podiatr Med Assoc 2006;96(5):428-436.
35. Campbell R S D, Grainger A J. Current concepts in imaging in tendinopathy. Clin Radiol 2001. 56253–267.267.
36. Stiell IG, McKnight RD, Greenberg GH, McDowell I, Nair RC, Wells GA, Johns C, Worthington JR. Implementation of the Ottawa Ankle Rules. Journal of the American Medical Association 1994; 271:827-832.
37. Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Reardon M, Stewart JP, Maloney J. Decision Rules for the Use of Radiography in Acute Ankle Injuries.Journal of the American Medical Association 1993; 269:1127-1132.
38. Stiell IG, Greenberg GH, McKnight RD, Nair RC, McDowell I, Worthington JR. A Study to Develop Clinical Decision Rules for the Use of Radiography in Acute Ankle Injuries. Annals of Emergency Medicine 1992; 21:384-390.
39. Movin T, Gad A, Reinholt FP. Tendon pathology in long-standing Achillodynia. Biopsy findings in 40 patients. Acta Orthop Scand1997;68:170–5.
40. Schwab SA. Epiphyseal injuries in the growing athlete. Can Med Assoc J 1977;117 : 626-630
41. Alfredson, H., Pietila, T., Jonsson, P., Lorentzon, R. (1998). Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. American Journal of Sports Medicine 26, 360–66.
42. Andres, Brett M.; Murrell, George A. C. (2008) Treatment of Tendinopathy: What Works, What Does Not, and What is on the Horizon Clinical Orthopaedics and Related Research 466(7)1539–1554
43. Anderson, D.L., Taunton, J.E., Davidson, R.G. (1992). Surgical management of chronic Achilles tendinitis. Clinical Journal of Sport Medicine 2, 38–42
44. Silbernagel KG, Thomee R, Thomee P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain--a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. Aug 2001;11(4):197-206.
45. Maffulli N, Walley G, Sayana MK, Longo UG, Denaro V. Eccentric calf muscle training in athletic patients with Achilles tendinopathy. Disabil Rehabil. 2008;30(20-22):1677-1684.
46. Allison GT, Purdam C. Eccentric loading for Achilles tendinopathy--strengthening or stretching? Br J Sports Med. Apr 2009;43(4):276-279.
47. Fahlstrom M, Jonsson P, Lorentzon R, Alfredson H. Chronic Achilles tendon pain treated with eccentric calf-muscle training. Knee Surg Sports Traumatol Arthrosc. Sep 2003;11(5):327-333.
48. Jonsson P, Wahlstrom P, Ohberg L, Alfredson H. Eccentric training in chronic painful impingement syndrome of the shoulder: results of a pilot study. Knee Surg Sports Traumatol Arthrosc. Jan 2006;14(1):76-81.
49. Josza L, Kannus P. Human Tendons. Champaign, IL: Human Kinetics; 1997.
50. Knobloch K, Schreibmueller L, Kraemer R, Jagodzinski M, Vogt PM, Redeker J. Gender and eccentric training in Achilles mid-portion tendinopathy. Knee Surg Sports Traumatol Arthrosc. May 2010;18(5):648-655.
51. Maffulli N, Khan KM, Puddu G. Overuse tendon conditions: time to change a confusing terminology. Arthroscopy. Nov-Dec 1998;14(8):840-843.
52. Mafi N, Lorentzon R, Alfredson H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee Surg Sports Traumatol Arthrosc. 2001;9(1):42-47.
53. Sayana MK, Maffulli N. Eccentric calf muscle training in non-athletic patients with Achilles tendinopathy. J Sci Med Sport. Feb 2007;10(1):52-58.
54. Adel Shalabi, A., Kristoffersen-Wilberg, Svensson, L., Aspelin, P., and Movin, T. Eccentric Training of the Gastrocnemius-Soleus Complex in Chronic Achilles Tendinopathy Results in Decreased Tendon Volume and Intratendinous Signal as Evaluated by MRI. American Journal of Sports Medicine (2004)
55. Yu, JaeHo; Park, DaeSung; Lee, GyuChang . Effect of eccentric strengthening on pain, muscle strength, endurance, and functional fitness factors in male patients with achilles tendinopathy. Am J Phys Med Rehabil. 2013 Jan;92(1):68-76.
56. Khan KM, Cook JL, Taunton JE, Bonar F. Overuse tendinosis, not tendonopathy part 1: a new paradigm for a difficult clinical problem. Phys Sportsmed. May 2000; 28(5):38-48.
57. Melham TJ, Sevier TL, Malnofski MJ, Wilson JK, Helfst RH. Chronic ankle pain and fibrosis successfully treated with a new non-invasive augmented soft tissue secondary to a history of repetitive use or excessive overload.
58. Dananberg, HJ, Shearstone, J, Guiliano, M “Manipulation Method for the Treatment of Ankle Equinus, “Journal of the American Podiatric Medical Association, 90:8 September, 2000 pp 385-389
59. Kilmartin TE, Wallace WA, Hill TW. Orthotic effect on metatarsophalangeal joint extension. J Am Podiatr Med Assoc 1991;81(8):414-417.
60. Saxena A, Ewen B, Maffulli N. Rehabilitation of the operated Achilles tendon: parameters for predicting return to activity. J Foot Ankle Surg 2011;50(1):37-40
62. Almekinders L, Temple J. Etiology, diagnosis, and treatment of tendonitis: an analysis of the literature. Med Sci Sports Exerc 1998. 301183– 1190.1190
63. Ryan, A.J. (1978). Injections for tendon injuries: Cure or cause. Physician and Sportsmedicine 6 (September), 39.
64. Shrier, I., Matheson, G.O., Kohl, H.W. (1996). Achilles tendonitis: Are corticosteroid injections useful or harmful? Clinical Journal of Sports Medicine 6, 245–50.
65. Alfredson H, Ohberg L. Sclerosing injections to areas of neo-vascularisation reduce pain in chronic achilles tendinopathy: A double-blind randomised controlled trial. Knee Surg Sports Traumatol Arthrosc. 2005;13(4):338–44.
66. Rompe JD, Nafe B, Furia JP, Maffulli N. Eccentric loading, shock-wave treatment, or a wait-and-see policy for tendinopathy of the main body of tendo achillis: A randomized controlled trial. Am J Sports Med. 2007;35(3):374–83
67. Alsousou J, Thompson M, Hulley P, Noble A, Willett K. The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: A review of the literature. J Bone Joint Surg Br. 2009;91(8):987–96.
68. Hawley JA. Handbook of Sports Medicine and Science, Running. Blackwell Science (2008) ISBN:9780470756874
69. Monto RR. Platelet rich plasma treatment for chronic Achilles tendinosis. Foot Ankle Int. 2012 May;33(5):379-85.
70. Schepull, Thorsten; Kvist, Joanna; Norrman, Hanna; Trinks, Marie; Berlin, Gösta; Aspenberg, Per (2011) Autologous Platelets Have No Effect on the Healing of Human Achilles Tendon Ruptures – A Randomized Single-Blind Study. American Journal of Sports Medicine vol. 39 no. 1 38-47
71. Nilsson-Helander K, et al. Acute Achilles Tendon Rupture: A Randomized, Controlled Study Comparing Surgical and Nonsurgical Treatments Using Validated Outcome Measures Am J Sports Med August 27, 2010
72. Weber, Martin; Niemann, Marco; Lanz, Renate; Müller, Thorsten (2003) Nonoperative Treatment of Acute Rupture of the Achilles Tendon – Results of a New Protocol and Comparison with Operative Treatment. The American Journal of Sports Medicine Sept. vol. 31 no. 5 685-691
73. Soroceanu A, Sidhw F, Aarabi S, Kaufman A, Glazebrook M, Surgical Versus Nonsurgical Treatment of Acute Achilles Tendon Rupture: A Meta- Analysis of Randomized Trials JBJS Vol 94 Issue 23
74. Stiell I, Wells G, Laupacis A, Brison R, Verbeek R, Vandemheen K, Naylor D. A multicentre trial to introduce clinical decision rules for the use of radiography in acute ankle injuries. British Medical Journal 1995; 311:594-597.
75. Anis AH, Stiell IG, Steward DF, Laupacis A. Cost-effectiveness analysis of the Ottawa Ankle Rules. Annals of Emergency Medicine 1995; 26:422-428.
76. Ryan M, Grau S, Krauss I, Maiwald C, Taunton J, Horstmann T. Kinematic analysis of runners with achilles mid-portion tendinopathy. Foot Ankle Int. 2009 Dec;30(12):1190-5
77. Knobloch K, Yoon U, Vogt PM Acute and overuse injuries correlated to hours of training in master running athletes Foot & Ankle International. American Orthopaedic Foot and Ankle Society [and] Swiss Foot and Ankle Society 2008, 29(7):671-676.
78. Davidson CJ, Ganion LR, Gehlsen GM, Verhoestra B, Roepke JE, Sevier TL. Rat tendon morphologic and functional changes resulting from soft tissue mobilization. Med Sci Sports Exerc. 1997;29:313-319
79. Gehlsen GM, Ganion LR, Helfst R. Fibroblast responses to variation in soft tissue mobilization pressure. Med Sci Sports Exerc. 1999;31:531- 535.
80. Loghmani MT, Warden S. Instrument-Assisted Cross-Fiber Massage Accelerates Knee Ligament Healing Orthop Sports Phys Ther 2009;39(7):506-514.
81. Uquillas CA, Guss MS, Ryan DJ, et al. Everything Achilles: Knowledge Update and Current Concepts in Management. J Bone Joint Surg Am. 2015;97:1187-95
82. Mani-Babu S, Morrissey D, Waugh C, Screen H, Barton C. The effectiveness of extracorporeal shock wave therapy in lower limb tendinopathy: a systematic review. Am J Sports Med. 2015 Mar;43(3):752-61.
83. Maffulli N, Papalia R, D’Adamio S, Diaz Balzani L, Denaro V. Pharmacological interventions for the treatment of Achilles tendinopathy: a systematic review of randomized controlled trials. Br Med Bull. 2015 Mar;113(1):101-15. Epub 2015 Jan 12.
84. Schepsis AA, Jones H, Haas AL. Achilles tendon disorders in athletes. Am J Sports Med. 2002 Mar-Apr;30(2):287-305.
85. Lantto I, Heikkinen J, Flinkkila T, Ohtonen P, Siira P, Laine V, Leppilahti J. A Prospective Randomized Trial Comparing Surgical and Nonsurgical Treatments of Acute Achilles Tendon Ruptures. Am J Sports Med. 2016 Sep;44(9):2406-14.
86. Spang C, Alfredson H, Docking SI, Masci L, Anderson G. The Plantaris Tendon. A Narrative Review Focusing On Anatomical Features And Clinical Importance. Bone Joint J 2016;98-B:1312–19.
87. Steenstra F, van Dijk CN. Achilles tendoscopy. Foot Ankle Clin 2006;11:429–438, viii.
88. Alfredson H. Midportion Achilles tendinosis and the plantaris tendon. Br J Sports Med 2011;45:1023–1025.
89. Calder JD, Freeman R, Pollock N. Plantaris excision in the treatment of non-inser- tional Achilles tendinopathy in elite athletes. Br J Sports Med 2015;49:1532–1534.
90. van Sterkenburg MN, van Dijk CN. Mid-portion Achilles tendinopathy: why painful? An evidence-based philosophy. Knee Surg Sports Traumatol Arthrosc 2011;19:1367–1375.
91. Dedes V, Stergioulas A, Kipreos G, Dede AM, Mitseas A, Panoutsopoulos GI. Effectiveness and Safety of Shockwave Therapy in Tendinopathies. Mater Sociomed. 2018 Jun;30(2):131-146. doi: 10.5455/msm.2018.30.141-146. 92. Cook JL, Purdam CR. The challenge of managing tendinopathy in competing athletes. Br J Sports Med. 2014;48:506-509.