

What is the Meniscus?
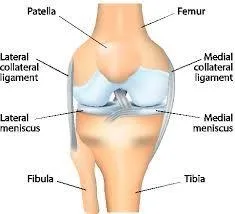
The knee meniscus is actually two shock-absorbent fibrocartilage discs (also called menisci) that form around the tibia and femur. The outer third of a meniscus has blood flow and nerve endings that are used to sense pain and positioning. The remainder of the meniscus does not have a blood supply and lacks nerve supply (2,3). Not surprisingly, healing potential is lower in the less vascular inner portion (28).
What does the meniscus do?
The meniscus plays an important role in knee biomechanics. The meniscus transmits 50-70% of compressive forces in full knee extension and up to 85% at 90 degrees bent (4). Other mechanical duties include shock absorption, synovial fluid distribution and lubrication (1).
Are meniscus injuries common?
Mensical injuries are fairly common. Males are affected more frequently at a rate of about 4:1 (3).
How do meniscus tears happen?
Meniscal tears are usually either “traumatic” or “degenerative”. Meniscal injuries may occur at any age. In children and adolescents, the meniscus is durable and rubbery so most injuries are “traumatic” as a result of a forceful rotational injury. As we age the meniscus grows weaker and less resilient, and “degenerative” tears become more likely, often resulting from simple or unrecognized causes (1,3,9). “Degenerative” tears are more common (1,3).

Is the inside or outside mensici most likely to tear?
The medial (inside) meniscus is damaged more often than the lateral meniscus (1).
Are meniscus tears associated wit mother knee injuries?
Approximately 1/3 of meniscal tears are associated with ACL injuries (9,10).
What are the symptoms of a meniscus tear?
Young patients often present following a sudden twist on a loaded (weight bearing) knee. Following acute injury, the patient may have difficulty with full weight bearing and may demonstrate an altered walking pattern. Older patients with degenerative injuries may not be able to report an event that caused their problem. Patients of any age usually complain of intermittent, movement-related pain, chiefly upon deep knee bends. Clicking, catching or locking, particularly between 20-45 degrees of extension, is common. The patient may report a sensation of giving-way or buckling. Patients may note tenderness along the joint line, slight knee swelling, and limited ROM in bending or knee extension. Deep squatting is usually uncomfortable (11).
Do I need X-rays or an MRI for a meniscus tear?
Plain film weight-bearing radiography may be needed to rule out fracture, osteochondral lesions, loose bodies and degenerative changes. (1) MRI is the most sensitive imaging modality for evaluation of menisci, but interpretation of MRI findings with regard to meniscal injuries may be confusing, and false positives are common. MRI exams reveal clinically irrelevant signal alterations or tears in 30- 36% of pain free patients (13,29). MRI imaging should be reserved for patients in whom arthroscopic surgery is anticipated (14).
What are the best treatment options for a meniscus tear?
Chiropractors can play an important role in the rehabilitation of most degenerative and some traumatic mensical injuries. Although the majority of acute tears in a young population will require surgery, 1/3 of these injuries may be treated non-surgically with full resolution (16).
For older patients with degenerative tears, a trial of conservative therapy is generally appropriate. Only about 6% of patients over the age of 40 require operative management (18). Patients with manageable pain and swelling, without loss of joint function, have shown functional improvement through conservative care equal to those who have undergone arthroscopic surgery (19).
What does conservative treatment include?
Initial conservative management should include rest, ice, compression and elevation (RICE).
Activity modification is essential to prevent further damage. Patients should avoid twisting on a weight-bearing, bent knee and may need to temporarily or permanently discontinue high-energy sports activity, like soccer or tennis. In some instances, a brace may be necessary to limit motion. Ice and anti-inflammatory modalities may help limit inflammation. NSAID’s may be appropriate in the initial stages (20).
Stretching and myofascial release techniques may be necessary for the surrounding muscles. IASTM of the knee capsule may provide benefit, as the meniscus has a shared attachment with this structure.
Manipulation may be necessary for restrictions in the ankle mortise joint, fibular head, hip, sacroiliac joints and spine.
Stationary bicycling, water walking and isometric strength training may be incorporated as swelling decreases. Dynamic exercises can be incorporated in as allowed, including knee bending, extension, and lunges.
Biomechanical deficits in hip or knee stability should be addressed, particularly gluteal weaknes and patellofemoral tracking disorders. Arch supports or orthotics may be necessary for patients who overpronate.
How does meniscus surgery affect you?
Surgical removal of meniscal tissue results in increased bony contact between the tibia and femur (7). Degenerative changes develop in nearly all post-meniscectomy patients (24). Degeneration seems to more common in those who have undergone lateral meniscectomy (25).
Rehabilitation of the knee pre and post surgery is essential to maintain proper quadriceps strength.
At Creekside Chiropractic & Performance Center, we are highly trained to treat meniscus tears conservatively. We are the only inter-disciplinary clinic providing services to Sheboygan, Sheboygan Falls, Plymouth, and Oostburg including chiropractic, manual therapy, myofascial release, ART (Active Release Technique), massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiropractor in Sheboygan by the Sheboygan Press.
Evidence Based-Patient Centered-Outcome Focused
Sources:
1. Goldblatt JP, Managing meniscal injuries: The diagnosis. J Musculoskel Med. 2009;26:343-351
2. Arnoczky SP, McDevitt CA. The meniscus: structure, function, repair, and replacement. In: Buckwalter JA, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2000:531-545.
3. Greis PE, Bardana DD, Holmstrom MC, Burks RT. Meniscal injury, I: basic science and evaluation. J Am Acad Orthop Surg. 2002;10:168-176
4. Rath E, Richmond JC. The menisci: basic science and advances in treatment. Br J Sports Med. 2000;34:252-257.
5. Packer JD, Rodeo SA. Meniscal allograft transplantation. Clin Sports Med. 2009:28:259-283, viii.
6. Levy IM, Torzilli PA, Warren RF. The effect of medial meniscectomy on anterior-posterior motion of the knee. J Bone Joint Surg. 1982;64A:883- 888.
7. Simon SR, Alaranta H, An KN, et al. Kinesiology. In: Buckwalter JA, Einhorn TA, Simon SR, eds. Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System. 2nd ed. Rosemont, IL: American Academy of Orthopaedic Surgeons; 2000:730-827.
9. Klimkiewicz JJ, Shaffer B. Meniscal surgery 2002 update: indications and techniques for resection, repair, regeneration, and replacement. Arthroscopy. 2002;18:14-25.
10. Kilcoyne KG et al Epidemiology of meniscal injury associated with ACL tears in young athletes”; The Cutting Edge, OrthoSuperSite; March 2012
11. Levy IM, Torzilli PA, Gould JD, Warren RF. The effect of lateral meniscectomy on motion of the knee. J Bone Joint Surg. 1989;71A:401-406.
12. Karachalios T, Hantes M, Zibis AH, et al. Diagnostic accuracy of a new clinical test (the Thessaly test) for early detection of meniscal tears. J Bone Joint Surg. 2005;87A:955-962.
13. Rath E, Richmond JC. The menisci: basic science and advances in treatment. Br J Sports Med. 2000;34:252-257.
14. Miller GK. A prospective study comparing the accuracy of the clinical diagnosis of meniscus tear with magnetic resonance imaging and its effect on clinical outcome. Arthroscopy. 1996;12:406-413.
15. Ciliz D, Ciliz A, Elverici E, et al. Evaluation of post-operative menisci with MR arthrography and routine conventional MRI. Clin Imaging. 2008;32:212-219
16. Goodwin Peter C, Effectiveness of supervised PTin the early period after arthroscopic partial menisectomy. Physical Therapy, 2003;83(6): 520- 535.
17. Saidoff David, McDonough Andrew. Critical Pathways in therapeutic intervention. Extremities and Spine; Philadelphia, PA:Mosby Inc., 2002: 611- 639.
18. Barrett GR, Field MH, Treacy SH, Ruff CG. Clinical results of meniscus repair in patients 40 years and older. Arthroscopy 1998;14:824–9.
19. Rimington T, Mallik K, Evans D, Mroczek K, Reider B. A prospective study of the nonoperative treatment of degenerative meniscus tears. Orthopedics 2009;32:8.
20. Lim HC, Bae JH, Wang JH, Seok CW, Kim MK. Non-operative treatment of degenerative posterior root tear of the medial meniscus. Knee Surg Sports Traumatol Arthrosc 2010;18:535–9.
21. Havard Osteras, Arthroscopic or conservative treatment of degenerative medial meniscal tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc. 24 August 2006
22. Matthews P, St-Pierre DM. Recovery of muscle strength following arthroscopic meniscectomy. J Orthop Sports Phys Ther. 1996;23:18–26
24. Andersson-Molina H, Karlsson H, Rockborn P. Arthroscopic partial and total meniscectomy: a long-term follow-up study with matched controls. Arthroscopy. 2002;18:183-189.
25. Salata MJ. A Systematic Review of Clinical Outcomes in Patients Undergoing Meniscectomy. American Journal of Sports Medicine. 2010 vol. 38 no. 9 1907-1916
26. Akseki D, Ozcan O, Boya H, Pinar H. A new weight-bearing meniscal test and a comparison with McMurray's test and joint line tenderness. Arthroscopy, 2004;20(9):951-958.
27. Chivers M, Howitt S. Anatomy and physical examination of the knee menisci: a narrative review of the orthopedic literature. J Can Chiropr Assoc, 2009;53(4):319-333.
28. Jeong H, Lee S, Ko C. Meniscectomy. Knee Surg Related Res, 2012;24(3):129-136.
29. Ryzewicz M, Peterson B, Siparsky P, Bartz R. The diagnosis of meniscus tears. Clin Orthop Related Res, 2007;455:123-133.