

The foot and ankle is a complex tool that has two roles; a shock absorber that contours to irregular surfaces, and a rigid propulsive lever. The ability of the foot to pronate plays an important role in the foot’s ability to multitask (1,2,3).

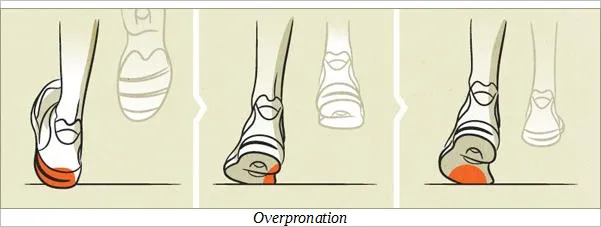
Foot pronation is the combined movement that results in flattening of the longitudinal arch of the foot (4). In a normal gait cycle, the process of pronation begins at heel strike, progresses through mid-stance and then reverts back toward supination to prepare a rigid lever for forward propulsion (4-7). In a healthy foot, pronation is limited to approximately 8 degrees (5-7). Movement beyond 8 degrees is termed “hyperpronation”.
What is the difference between hyperpronation and "flat feet"?
At a glance, they look the same, but indeed they are different. Hyperpronation is dynamic, meaning that it is during the active process during movement. Someone who has flat feet is extremely likely to hyperpronate, but it is not necessary for someone who hyperpronates to have "flat feet" (pes planus).
What happens if I hyperpronate?
The repetitive stress of hyperpronation causes significant strain on the soft tissues of the foot. Chronic hyperpronation may result in a pathologic laxity of the calcaneonavicular ligament in the foot and the talonavicular joint. (63) The relatively inelastic medial band of the plantar fascia is often stressed beyond its capacity to elongate, causing irritation in those who hyperpronate (10). Traction from hyperprontion contributes to posterior tibial tendinopathy and posterior tibial nerve irritation (also known as tarsal tunnel syndrome) (11).
The effects of hyperpronation are not localized to the foot. Hyperpronation causes internal rotation of the tibia (12), which creates a torque that continues up the kinetic chain and results in internal rotation of the femur, which moves the femoral head and acetabulum backward, causing anterior tilt of the pelvis, and hyperextension of the lumbar spine (7,8,14,15).
Does hyperpronation affect the knee?
Hyperpronation also stresses the knee through a number of mechanisms. In particular, a lowered arch combined with internal tibial rotation places significant stress on the inside portion of the knee (8). This challenges the medial collateral ligament and anterior cruciate ligament and is a well-recognized contributor to injuries of these structures (16,17). Additionally, internal rotation of the tibia and femur cause a relative lateral displacement of the patella, pushing the patellar facet into the lateral femoral condyle (18). Not surprisingly, low arches and hyperpronation are commonly associated with knee pain (19-22). Longstanding misalignment of the patellofemoral joint is associated with degeneration of the knee (19,22,23).
How does hyperpronation affect the hip?
Not all of the torsional energy of tibial internal rotation is dissipated by the knee. In fact, much of it travels through the knee into the thigh, and is absorbed by the hip (18). Internal rotation of the femur has a detrimental effect on several muscle groups, including the quadriceps, hip adductors, and hip abductors, such as the gluteus medius (8). Foot hyperpronation and hip abductor weakness are known biomechanical coconspirators. In a self-perpetuating cycle, the compensatory changes that occur upstream in response to hyperpronation end up increasing hyperpronation and vice versa.
How does hyperpronation affect the lower back?
Internal rotation of the femur (hip) causes the pelvis to shift anteriorly (8). This further contributes to “stretch weakening” of the gluteal and abdominal muscles and adaptive tightening of the hip flexors (lower crossed syndrome). This process limits hip extension, which in turn increases extension forces on the lumbar spine facets (8). What’s more, the functional leg length inequality of a unilateral flat foot may cause lateral bending of the lumbar spine toward the affected side, further increasing facet compression (8). As expected, hyperpronation contributes to lower back pain (14,25-32).
How does our body adapt to hyperpronation?
The body employs many compensatory mechanisms to offset foot hyperpronation – although these corrections do not come without a cost (8). Foot hyperpronation ultimately causes joints higher in the kinetic chain to absorb more shock (8,20,21,30). The increased load on the knees, hip, and spine is compounded during athletic activity, particularly running and jumping.
Can you have hyperpronation but not have any pain?
While the “functional” diagnosis of foot hyperpronation can present asymptomatically (pain free), it is a well-known contributor to a multitude of painful “structural” diagnoses throughout the lower body.
What is the typical presentation of foot hyperpronation?
There is no “typical” presentation for foot hyperpronation, but the condition should be considered in any person with leg, ankle, or foot pain, particularly those with plantar fasciitis, Achilles tendinopathy, metarsalgia, medial tibial stress syndrome, patellofemoral pain syndrome, greater trochanteric pain syndrome, and low back pain. Longstanding hyperpronation may lead to ligamentous laxity and degeneration of affected joints (19-23,39,40).
How is hyperpronation managed?
The management of foot hyperpronation includes prescribing arch supports as well as exercises to control motion at the hip and ankle (35). Factors, including the degree of hyperpronation and the functional demands of the patient, will dictate whether custom or prefabricated orthotics are most appropriate. Flexible full-length orthotics have been shown to improve Q angles in patients who hyperpronate and may aid in the treatment of secondary biomechanical problems associated with foot hyperpronation, including foot pain, knee pain, and low back pain (45,46).
However, excess bulky orthotics or shoes with excessive cushioning may have an adverse effect on proprioception and balance (47).
Are leg length inequalities part of the issue?
Those with hyperpronation should address the possibility of standing leg length inequalities (48,49). Unilateral hyperpronation may cause a functional leg length inequality, increasing the risk of degeneration on the short side and stress fracture on the long side (50,51). Confirmed leg length inequalities must be addressed (51-53).
Should stretching exercises be utilized?
Yes. Inadequate ankle dorsiflexion may force excessive pronation through the mid foot. Stretching exercises and myofascial release may be appropriate for restrictions in the gastroc and soleus (calf) muscles.
What about strengthening exercises for hyperpronation?
Strengthening exercises should be directed at the foot and hip, specifically the posterior tibialis and hip abductor muscles. Traditional strength training does not necessarily change faulty movement patterns (54).
Exercise programs should incorporate proprioception, beginning with simple balance training like a single leg stance or Vele’s, then progressing to lunges on an unstable surface, like a Bosu ball (55-58). Strengthening exercises for the hip abductors could include a posterior lunge, clam with band, lateral band walks, or sidebridge.
Inward collapse of the knee, regardless of cause, is associated with ACL injury. Athletes with inward collapse (valgus stress) will benefit from warm-up drills. (59-61).
Are there other factors that affect hyperpronation?
Obesity exacerbates hyperpronation therefore diet and exercise recommendations are be appropriate for overweight patients (64,65). Hyperpronators should avoid shoes with narrow toe boxes or high heels (11).
My child has flat feet and hyperpronates, is that normal?
Of note- hyperpronation is common in children, as development of the longitudinal arch is usually not complete until the age of 8 (41). Some studies suggest that shoe wear in children is detrimental to the development of a healthy longitudinal arch (62,63).
At Creekside Chiropractic & Performance Center, we are highly trained to treat over pronation. We are the only inter-disciplinary clinic providing services to Sheboygan, Sheboygan Falls, Plymouth, and Oostburg including chiropractic, manual therapy, myofascial release, ART (Active Release Technique), massage therapy, acupuncture, physiotherapy, rehabilitative exercise, nutritional counseling, personal training, and golf performance training under one roof. We also offer fully customized orthotics to assist patient's in this condition. Utilizing these different services, we can help patients and clients reach the best outcomes and the best versions of themselves. Voted Best Chiropractor in Sheboygan by the Sheboygan Press.
Evidence Based-Patient Centered-Outcome Focused
Sources:
1. Waerlop I, Allen S. Pedographs and Gait Analysis: Case Studies and Clinical Pearls. Victoria, BC, Canada: Trafford, 2006.
2. Michaud T. Foot Orthoses and Other Forms of Conservative Foot Care. Newton Mass.: Michaud, 1993:29.
3. Phillips RD, Phillips RL. Quantative analysis of the locking mechanism of the midtarsal joint. J Am Pod Med Assoc, 1983;73:518-22.
4. Minkowsky R. The spine, an integral part of the lower extremity. In: Clinical Biomechanics of the Lower Extremities, Valmassey R. St Louis: Mosby, 1996:105.
5. Close JR, Inman VT, Poor PM, Todd FN. The function of the subtalar joint. Clin Orthop, 1967;50(1-2):159-79.
6. Wright DG, Desai SM, Henderson WH. Action of the subtalar and ankle joint complex during the stance phase of walking. J Bone Joint Surg, 1964;46A(2):361-82.
7. Perry J. Gait Analysis: Normal and Pathological Function. Thorofare, NJ: Slack, 1992:73.
8. Allen S, Waerlop IF, Lardner R. A Few Words About Pronation Dynamic Chiropractic – February 26, 2008, Vol. 26, Issue 05
9. Michaud TC Development of the arch: Functional implications Lower Extremeity Review Accessed 11/12/14: http://lermagazine.com/article...
10. Manter JT. Movements of the subtalar and transverse tarsal joints. Anat Rec 1941;80(4):397-409.
11. Stovitz SD, Coetzee JC. Hyperpronation and Foot Pain. The Physician and Sportsmedicine- Vol. 32 - No. 8 - August 2004
12. Mann RA, Baxter DE, Lutter LD. Running symposium. Foot Ankle, 1981;1(4):190-224.
14. Cibulka MT. Low back pain and its relation to the hip and foot. J Orthop Sports Phys Ther, October 1999;29(10):595-601.
15. Michaud T. Foot Orthoses and Other Forms of Conservative Foot Care. Newton, Mass.: Michaud, 1993;59-62.
16. McLean SG, Huang X, Su A, Van Den Bogert AJ. Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clin Biomech 2004;19(8):828-838.
17. Loudon JK, Jenkins W, Loudon KL. The relationship between static posture and ACL injuries in female athletes. J Orthop Sports Phys Ther 1996;24(2):91-97.
18. Lafortune MA, Cavanagh PR, Sommer HJ, Kalenak A. Foot inversion-eversion and knee kinematics during walking. J Orthop Res 1994;12(3):412-420.
19. Klingman RE. Foot pronation and patellofemoral joint function. J Orthop Sports Phys Ther, 1999;29(7):421.
20. Zammit GV, Payne CB. Relationship between positive clinical outcomes of foot orthotic treatment and changes in rearfoot kinematics. J Am Podiatr Med Assoc, May - June 2007;97(3):207-12.
21. Root RC, Orien WP, Weed JH. Normal and abnormal function of the foot. Clinical Biomechanics, 1977.
22. Rothbart BA, Estabrook L. Excessive pronation: a major biomechanical determinant in the development of chondromalacia and pelvic lists. J Manipulative Physiol Ther, 1988;11(5):373-9.
23. Ross FD. The relationship of abnormal foot pronation to hallux abducto valgus - a pilot study. Prosthet Orthot Int, August 1986;10(2):72-8.
25. Michaud T. Foot orthoses and other forms of conservative foot care. 2nd ed: Thomas Michaud; 1997. p 56-70, 89, 114-17
26. Dananberg HJ, Guiliano M. Chronic low-back pain and its response to custom-made foot orthoses. J Am Podiatr Med Assoc 1999;89:109-17
27. Larsen K, Weidich F, Leboeuf-Yde C. Can custom-made biomechanic shoe orthoses prevent problems in the back and lower extremities? A randomized, controlled intervention trial of 146 military conscripts. J Manipulative Physiol Ther 2002; 25:326-31.
28. Cibulka MT. Low back pain and its relation to the hip and foot. J Orthop Sports Phys Ther, October 1999;29(10):595-601.
29. Waerlop I, Allen S. Pedographs and Gait Analysis: Case Studies and Clinical Pearls. Victoria, BC, Canada: Trafford, 2006.
30. Botte RR. An interpretation of the pronation syndrome and foot types of patients with low back pain. J Am Podiatr Med Assoc, May 1981;71(5):243-53.
31. Root RC, Orien WP, Weed JH. Normal and abnormal function of the foot. Clinical Biomechanics, 1977.
33. Williams DS, McClay IS, Hamill J, Buchanan TS. Lower extremity kinematic and kinetic differences in runners with high and low arches. J Appl Biomech 2001;17(2):153-63. Manter JT. Movements of the subtalar and transverse tarsal joints. Anat Rec 1941;80(4):397-409.
34. Messier SP, Pittala KA. Etiologic factors associated with selected running injuries. Med Sci Sports Exerc 1988;20(5):501-505.
35. Michaud TC. Development of the Arch: Functioal Implications. Lower Extremity Review.July 2012. http://lermagazine.com/article/developmnt- of-the-arch-functional-implications . Accessed 11/28/14
38. Allen S, Waerlop IF, Lardner R. A Few Words About Pronation Dynamic Chiropractic – February 26, 2008, Vol. 26, Issue 05
39. Woodford-Rogers B, Cyphert L, Denegar CR. Risk factors for anterior cruciate ligament injury in high school and college athletes. J Athl Train, 1994;29(4):343-6.
40. Krivickas LS. Anatomical factors associated with overuse sports injuries. Sports Med, 1997;24(2):132-46.
41. Gould N, Moreland M, Alvarez R, et al. Development of the child’s arch. Foot Ankle 1989;9(5):241-245.
42. Shrader JA, Popovich JM, Gracey GC, Danoff JV. Navicular drop measurement in people with rheumatoid arthritis: interrater and intrarater reliability. Phys Ther 2005;85:656-64.
43. Brantingham JW, Gilbert J, Shaik J, Globe G. Sagittal plane blockage of the foot, ankle and hallux and foot alignment— prevalence and association with low back pain. J Chiropr Med 2006;5:123-7.
45. Menz HB, Dufour AB, Riskowski JL, Hillstrom HJ, Hannan MT. Foot posture, foot function and low back pain: the Framingham Foot Study. Rheumatology (Oxford). 2013 Dec;52(12):2275-82. doi: 10.1093/rheumatology/ket298. Epub 2013 Sep 17.
46. Robert Kuhn, Terry R. Yochum, Anton R. Cherry, and Sean S. Rodgers Immediate Changes in the quadriceps Femoris Angle After Insertion of an Orthotic Device J Manipulative Physiol Ther 2002;25:465 70
47. Robbins SE, Hanna AM. Running-related injury prevention through barefoot adaptations. Med Sci Sports Exerc. 1987;19:148-156.
48. . Ridola C, Palma A, Cappello F, et al. Symmetry of healthy adult feet: role of orthostatic footprint at computerized baropodometry and of digital formula. Ital J Anat Embryol 2001;106:99-112.
49. Sforza C, Michielon G, Fragnito N, Ferrario VF. Foot asymmetry in healthy adults: elliptic Fourier analysis of standardized footprints. J Orthop Res 1998;758-65.
50. Friberg O. Leg length asymmetry in stress fractures: a clinical and radiographic study. J Sports Med Phys Fitness. 1982;22:485-488.
51. Harvey W, Yang M, Cooke T, et al. Associations of leg-length inequality with prevalent, incident, and progressive knee osteoarthritis: a cohort study. Ann Intern Med. 2010;152:287-295.
52. Giles I, Taylor J. Lumbar spine structural changes associated with leg-length inequality. Spine 1982;7:159-162.
53. Pertunnen J, Antilla E, Sodergtard J et al. Gait asymmetry in patients with limb-length discrepancies. Scand J Med Sci Sports. 2004;14:49-56
54. Willy R, Davis I. The effect of a hip-strengthening program on mechanics during running and during a single-leg squat. J Orthop Sports Phys Ther 2011;41(9):625-632.
55. Rotem-Lehrer N, Laufer Y. Effect of focus of attention on transfer of a postural control task following an ankle sprain. J Orthop Sports Phys Ther. 2007;37:564-569.
56. McNevin NH, Wulf G. Attentional focus on suprapostural tasks affects postural control. Hum Mov Sci. 2002;21:187-202.
57. McNevin N, Wulf G, Carlson C. Effects of attentional focus, self-control, and dyad training on motor learning: implications for physical rehabilitation. Phys Ther. 2000;80:373-385.
59. Gilchrist J, Mandelbaum BR, Melancon H, et al. A randomized controlled trial to prevent noncontact anterior cruciate ligament injury in female collegiate soccer players. Am J Sports Med 2008;36(8):1476-1483.
60. Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med 1999;27(6):699-706.
61. LaBella CR, Huxford MR, Grissom J, et al. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: cluster randomized controlled trial. Arch Pediatr Adolesc Med 2011;165(11):1033-1040.
62. Rao UB, Joseph B: The influence of footwear on the prevalence of flat foot: a survey of 2300 children. J Bone Joint Surg Br 1992;74(4):525-527
63. Sachithanandam V, Joseph B: The influence of footwear on the prevalence of flat foot: a survey of 1846 skeletally mature persons. J Bone Joint Surg Br 1995;77(2):254-257
64. Messier SP, Davies AB, Moore DT, et al: Severe obesity: effects on foot mechanics during walking. Foot Ankle Int 1994;15(1):29-34
65. Hills AP, Hennig EM, McDonald M, et al: Plantar pressure differences between obese and non-obese adults: a biomechanical analysis. Int J Obes Relat Metab Disord 2001;25 (11):1674-1679
66. Williams DS, McClay IS, Hamill J. Arch structure and injury patterns in runners. Clin Biomech 2001;16(4):341-347. 67. Williams D, McClay I, Hamill J. Arch structure and injury patterns in runners. Clin Biomech, 2001;16:341-347.
68. Williams D, McClay I. Measurements used to characterize the foot and the medial longitudinal arch: reliability and validity. Phys Ther, 2000;80:864-871.
69. Franettovich M, McPoil T, Russell T, et al. The ability to predict dynamic foot posture from static measurements. J Am Podiatr Med Assoc, 2007;97:115.